





Updated: The Zika Virus Information from the CDC; Science Friday (PRI, NPR) & World Health Organization Convenes Emergency Meeting
Editor's Note: We realize that few senior womenwill be pregnant during this outbreak time, but we have daughters, friends, nieces who may be. Update: World Health Organization; there is also a segment at PRI's Science Friday on the mosquito and the virus, Americas Brace for Zika Spread. We're including an Asian Tiger Mosquito release from the US Department of Agriculture.

WHO Director-General, Margaret Chan, will convene an International Health Regulations Emergency Committee on Zika virus and observed increase in neurological disorders and neonatal malformations. The Committee will meet on Monday 1 February in Geneva to ascertain whether the outbreak constitutes a Public Health Emergency of International Concern.
Interim Guidelines for Pregnant Women During a Zika Virus Outbreak — United States, 2016 Weekly / January 22, 2016 /
CDC has developed interim guidelines for health care providers in the United States caring for pregnant women during a Zika virus outbreak. These guidelines include recommendations for pregnant women considering travel to an area with Zika virus transmission and recommendations for screening, testing, and management of pregnant returning travelers. Updates on areas with ongoing Zika virus transmission are available online (http://wwwnc.cdc.gov/travel/notices/). Health care providers should ask all pregnant women about recent travel. Pregnant women with a history of travel to an area with Zika virus transmission and who report two or more symptoms consistent with Zika virus disease (acute onset of fever, maculopapular rash, arthralgia, or conjunctivitis) during or within 2 weeks of travel, or who have ultrasound findings of fetal microcephaly or intracranial calcifications, should be tested for Zika virus infection in consultation with their state or local health department. Testing is not indicated for women without a travel history to an area with Zika virus transmission. In pregnant women with laboratory evidence of Zika virus infection, serial ultrasound examination should be considered to monitor fetal growth and anatomy and referral to a maternal-fetal medicine or infectious disease specialist with expertise in pregnancy management is recommended. There is no specific antiviral treatment for Zika virus; supportive care is recommended.
Pregnant women can be infected with Zika virus in any trimester. The incidence of Zika virus infection in pregnant women is not currently known, and data on pregnant women infected with Zika virus are limited. No evidence exists to suggest that pregnant women are more susceptible to Zika virus infection or experience more severe disease during pregnancy.
Aedes aegypti mosquito
Maternal-fetal transmission of Zika virus has been documented throughout pregnancy (4,7,8). Although Zika virus RNA has been detected in the pathologic specimens of fetal losses (4), it is not known if Zika virus caused the fetal losses. Zika virus infections have been confirmed in infants with microcephaly (4), and in the current outbreak in Brazil, a marked increase in the number of infants born with microcephaly has been reported (9). However, it is not known how many of the microcephaly cases are associated with Zika virus infection. Studies are under way to investigate the association of Zika virus infection and microcephaly, including the role of other contributory factors (e.g., prior or concurrent infection with other organisms, nutrition, and environment). The full spectrum of outcomes that might be associated with Zika virus infections during pregnancy is unknown and requires further investigation.
Recommendations for Pregnant Women Considering Travel to an Area of Zika Virus Transmission
Because there is neither a vaccine nor prophylactic medications available to prevent Zika virus infection, CDC recommends that all pregnant women consider postponing travel to areas where Zika virus transmission is ongoing (10). If a pregnant woman travels to an area with Zika virus transmission, she should be advised to strictly follow steps to avoid mosquito bites (11,12). Mosquitoes that spread Zika virus bite both indoors and outdoors, mostly during the daytime; therefore, it is important to ensure protection from mosquitoes throughout the entire day (13). Mosquito prevention strategies include wearing long-sleeved shirts and long pants, using U.S. Environmental Protection Agency (EPA) — registered insect repellents, using permethrin-treated clothing and gear, and staying and sleeping in screened-in or air-conditioned rooms. When used as directed on the product label, insect repellents containing DEET, picaridin, and IR3535 are safe for pregnant women (14,15). Further guidelines for using insect repellents are available online (http://wwwnc.cdc.gov/travel/page/avoid-bug-bites) (11,15).
Recommendations for Pregnant Women with History of Travel to an Area of Zika Virus Transmission
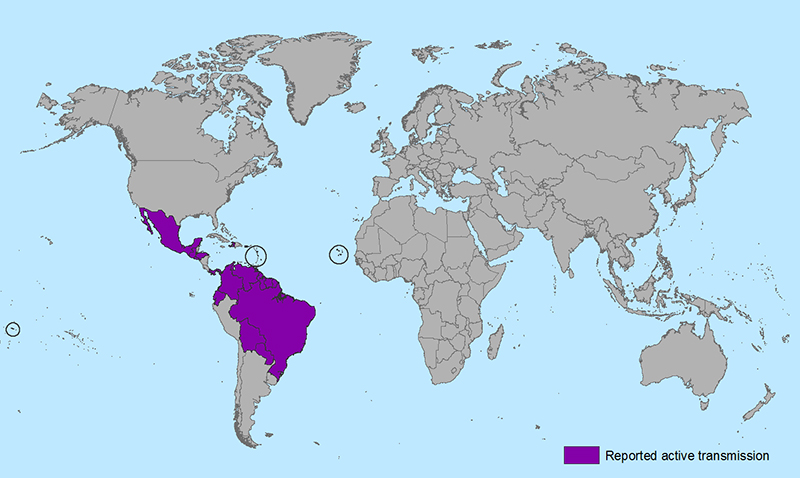
Health care providers should ask all pregnant women about recent travel. Women who traveled to an area with ongoing Zika virus transmission during pregnancy should be evaluated for Zika virus infection and tested in accordance with CDC Interim Guidance (Figure). Because of the similar geographic distribution and clinical presentation of Zika, dengue, and chikungunya virus infection, patients with symptoms consistent with Zika virus disease should also be evaluated for dengue and chikungunya virus infection, in accordance with existing guidelines (16,17).
Zika virus testing of maternal serum includes reverse transcription-polymerase chain reaction (RT-PCR) testing for symptomatic patients with onset of symptoms within the previous week. Immunoglobulin M (IgM) and neutralizing antibody testing should be performed on specimens collected ≥4 days after onset of symptoms. Cross-reaction with related flaviviruses (e.g., dengue or yellow fever) is common with antibody testing, and thus it might be difficult to distinguish Zika virus infection from other flavivirus infections. Consultation with state or local health departments might be necessary to assist with interpretation of results (18). Testing of asymptomatic pregnant women is not recommended in the absence of fetal microcephaly or intracranial calcifications.
Zika virus RT-PCR testing can be performed on amniotic fluid (7,9). Currently, it is unknown how sensitive or specific this test is for congenital infection. Also, it is unknown if a positive result is predictive of a subsequent fetal abnormality, and if so, what proportion of infants born after infection will have abnormalities. Amniocentesis is associated with an overall 0.1% risk of pregnancy loss when performed at less than 24 weeks of gestation (19). Amniocentesis performed ≥15 weeks of gestation is associated with lower rates of complications than those performed at earlier gestational ages, and early amniocentesis (≤14 weeks of gestation) is not recommended (20). Health care providers should discuss the risks and benefits of amniocentesis with their patients. A positive RT-PCR result on amniotic fluid would be suggestive of intrauterine infection and potentially useful to pregnant women and their health care providers (20).
For a live birth with evidence of maternal or fetal Zika virus infection, the following tests are recommended: histopathologic examination of the placenta and umbilical cord; testing of frozen placental tissue and cord tissue for Zika virus RNA; and testing of cord serum for Zika and dengue virus IgM and neutralizing antibodies. CDC is developing guidelines for infants infected by Zika virus. If a pregnancy results in a fetal loss in a woman with history of travel to an area of Zika virus transmission with symptoms consistent with Zika virus disease during or within 2 weeks of travel or findings of fetal microcephaly, Zika virus RT-PCR and immunohistochemical staining should be performed on fetal tissues, including umbilical cord and placenta.
There is no commercially available test for Zika virus. Testing for Zika virus infection is performed at CDC and several state health departments. Health care providers should contact their state or local health department to facilitate testing and for assistance with interpreting results (4).
How to Treat Pregnant Women with Diagnoses of Zika Virus Disease
No specific antiviral treatment is available for Zika virus disease. Treatment is generally supportive and can include rest, fluids, and use of analgesics and antipyretics (4). Fever should be treated with acetaminophen (21). Although aspirin and other nonsteroidal anti-inflammatory drugs are not typically used in pregnancy, these medications should specifically be avoided until dengue can be ruled out to reduce the risk for hemorrhage (4,9,17).
In a pregnant woman with laboratory evidence of Zika virus in serum or amniotic fluid, serial ultrasounds should be considered to monitor fetal anatomy and growth every 3–4 weeks. Referral to a maternal-fetal medicine or infectious disease specialist with expertise in pregnancy management is recommended.
More Articles
- National Institutes of Health: Common Misconceptions About Vitamins and Minerals
- A Yale Medicine Doctor Explains How Naloxone, a Medication That Reverses an Opioid Overdose, Works
- Kaiser Health News Research Roundup: Pan-Coronavirus Vaccine; Long Covid; Supplemental Vitamin D; Cell Movement
- How They Did It: Tampa Bay Times Reporters Expose High Airborne Lead Levels at Florida Recycling Factory
- A Scout Report Selection: Science-Based Medicine
- Journalist's Resource: Religious Exemptions and Required Vaccines; Examining the Research
- Government of Canada Renews Investment in Largest Canadian Study on Aging
- Kaiser Health News: Paying Billions for Controversial Alzheimer’s Drug? How About Funding This Instead?
- Medicare Covers FDA-approved COVID-19 Vaccines; You Pay Nothing For the COVID-19 Vaccine
- Envision Color: Activity Patterns in the Brain are Specific to the Color You See; NIH Research Findings Reveal New Aspects of Visual Processing